A Historical Perspective of Nurses in Prisons
A History of Prisons & Jails
http://www.easternstate.org/explore/flickr?page=6
A historical overview of the experiences and challenges of correctional RNs cannot be described in isolation from the strongly influential context of correctional facilities throughout the years. Instead, a comprehensive account of the history of correctional nursing must be considered alongside prisoners’ continuous plight for their healthcare rights (Dumpel, 2005). As far back as the 1800s, it was clear that penitentiaries demonstrated issues with their priority purposes and their suboptimal conditions of confinement and security (Dumpel, 2005).
Much of the literature on health care within correctional facilities is based on American correctional systems. Dumpel (2005) explains that in 1929, a report was published by the National Society for Penal Information which reflected the results of field surveys regarding health care within American prisons. This report detailed the prisons’ vast shortage and inadequacy of (Dumpel, 2005):
Ø Hospital facilities
Ø Equipment
Ø Personnel
Ø Resources
Furthermore, this report promoted and supported the notion of rehabilitation as the priority goal within correctional facilities (Dumpel, 2005). It also highlighted the need to standardize health practices (Dumpel, 2005). Yet, despite the recommendations put forth by this report, administrators of penitentiaries have vastly dismissed rehabilitation as the purpose and goal of prisons (Dumpel, 2005). Therefore, as described by Dumpel (2005), the “quasi-military management style” (p. 22) within penitentiaries has largely predominated since the 1940s. Since then, order and security have taken precedence over any other areas within prisons, including health care services, which are largely perceived as counterproductive to the priority goal of security (Dumpel, 2005). In fact, in 1975, one researcher even reported that correctional nurses are “disruptive to prison goals” (Dumpel, 2005, p. 22).
In view of this historical perspective, it is not surprising that predominant attitudes towards inmates have reflected biased notions such as (Dumpel, 2005):
Ø Prisoners having a tendency to “fake” illness
Ø It is acceptable to remain indifferent to prisoners’ healthcare needs
Ø Prisoners being underserving of basic human considerations
Not only were these prevalent attitudes deeply embedded into the culture of correctional facilities, but staff members (such as custody officers) within prisons also collectively felt that only inmates who are in most obvious and dire need of health care may or may not have access to it (Dumpel, 2005). It is clear that the driving force within prisons was one of power struggle and distrust between prisoners and correctional staff (Dumpel, 2005).
Much of the literature on health care within correctional facilities is based on American correctional systems. Dumpel (2005) explains that in 1929, a report was published by the National Society for Penal Information which reflected the results of field surveys regarding health care within American prisons. This report detailed the prisons’ vast shortage and inadequacy of (Dumpel, 2005):
Ø Hospital facilities
Ø Equipment
Ø Personnel
Ø Resources
Furthermore, this report promoted and supported the notion of rehabilitation as the priority goal within correctional facilities (Dumpel, 2005). It also highlighted the need to standardize health practices (Dumpel, 2005). Yet, despite the recommendations put forth by this report, administrators of penitentiaries have vastly dismissed rehabilitation as the purpose and goal of prisons (Dumpel, 2005). Therefore, as described by Dumpel (2005), the “quasi-military management style” (p. 22) within penitentiaries has largely predominated since the 1940s. Since then, order and security have taken precedence over any other areas within prisons, including health care services, which are largely perceived as counterproductive to the priority goal of security (Dumpel, 2005). In fact, in 1975, one researcher even reported that correctional nurses are “disruptive to prison goals” (Dumpel, 2005, p. 22).
In view of this historical perspective, it is not surprising that predominant attitudes towards inmates have reflected biased notions such as (Dumpel, 2005):
Ø Prisoners having a tendency to “fake” illness
Ø It is acceptable to remain indifferent to prisoners’ healthcare needs
Ø Prisoners being underserving of basic human considerations
Not only were these prevalent attitudes deeply embedded into the culture of correctional facilities, but staff members (such as custody officers) within prisons also collectively felt that only inmates who are in most obvious and dire need of health care may or may not have access to it (Dumpel, 2005). It is clear that the driving force within prisons was one of power struggle and distrust between prisoners and correctional staff (Dumpel, 2005).
The Enforcement of Inmates' Right to Healthcare
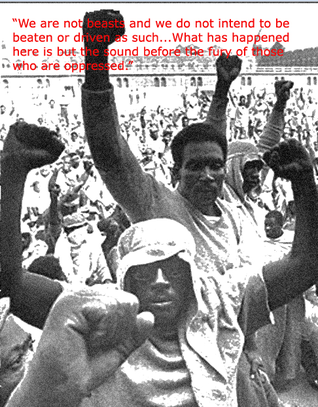
http://www.onthisdeity.com/9th-september-1971-%E2%80%93-the-attica-state-prison-riot/
In 1971, the Attica State Prison situated in New York experienced an uprising that led to the death of 43 prisoners and guards (Dumpel, 2005). This rebellion was in part initiated by protests against poor health care and sparked a subsequent flood of inmate lawsuits, which eventually led to the United States Supreme Court to declare in 1976 that “failure to provide adequate health care to individuals confined in correctional institutions violated prisoners’ constitutional rights” (Weiskopf, 2005, p. 336). This means that once a person is imprisoned, he or she must be provided minimum and adequate health care that is comparable to the services received by the general population (Dumpel, 2005).
Thus, all through the 1970s, correctional facilities experienced drastic improvements in their provision of health services (Weiskopf, 2005). Furthermore, in 1990, the United Nations declared in the Basic Principles of the Treatment of Prisoners that inmates would receive access to available health care services “without discrimination on the grounds of their legal situation” (Condon, Harris, Kemple, & Powell, 2010, p. 1258). Prisoners’ healthcare rights include the right to (Dumpel, 2005):
o Access care
o Refuse care
o Confidentiality
o Informed consent
o Privacy
Meanwhile, between 1980 and 1995, prison systems experienced a massive increase in their inmate population, which more than tripled, in large part due to mandatory sentences for drug offences (Weiskopf, 2005). The result of this was overcrowding to a critical level, and an escalating demand for health care services within correctional facilities (Weiskopf, 2005).
Thus, all through the 1970s, correctional facilities experienced drastic improvements in their provision of health services (Weiskopf, 2005). Furthermore, in 1990, the United Nations declared in the Basic Principles of the Treatment of Prisoners that inmates would receive access to available health care services “without discrimination on the grounds of their legal situation” (Condon, Harris, Kemple, & Powell, 2010, p. 1258). Prisoners’ healthcare rights include the right to (Dumpel, 2005):
o Access care
o Refuse care
o Confidentiality
o Informed consent
o Privacy
Meanwhile, between 1980 and 1995, prison systems experienced a massive increase in their inmate population, which more than tripled, in large part due to mandatory sentences for drug offences (Weiskopf, 2005). The result of this was overcrowding to a critical level, and an escalating demand for health care services within correctional facilities (Weiskopf, 2005).
California Department of Corrections & Rehabilitation
http://www.americawear.com/Cdcr-Patch.html
The largest prison system in the U.S. is situated in California (Dumpel, 2006). Yet, it is concerning to learn that its prison system does not follow current nationally-established standards (Dumpel, 2006). Moreover, there are numerous political and other forces that influence its correctional system, including amongst them (Dumpel, 2006):
Ø The government
Ø The California Correctional Peace Officers Associatio (CCPOA)
Ø The prison guards' union
Ø The Department of Corrections and Rehabilitation itself (CDCR)
The CDCR represents a sizable state agency that has been known to have its own agenda (Dumpel, 2006). For instance, press reports have recently shed light on some major underlying ethical issues with the CDCR such as the “code of silence” that is upheld by prison staff (Dumpel, 2006). In fact, each of the aforementioned bodies with their own area of responsibilities often have conflicting interests (Dumpel, 2006). The pursuit of their individual goals often results in the abuse of public trust and failure to meet the needs of inmates (Dumpel, 2006). In this highly political milieu, CDCR employees (including correctional RNs) strongly lack a meaningful voice within the system (Dumpel, 2006). To make matters worse, the poor condition of the system is exacerbated by the combination of these powerful interest groups and a heavily deficient budget (Dumpel, 2006). The pervasive lack of structure within government bodies that run health services create great challenges for those wishing to advocate for inmates and combat political forces that impact their rights to health care (Dumpel, 2006).
Several lawsuits against the CDCR outlined serious issues in areas such as (Dumpel, 2006):
Ø Improper screening of prisoners
Ø Staffing
Ø Incompetence with health care practices
Ø Access to care
Ø Medical records
Ø Implementing basic protocols
Ø Delays in care
Ø Pharmacy and medication management
Despite abundant legal action regarding prisoners’ health care in the past 20 years, it appears that “real and lasting improvements have yet to be achieved” (Dumpel, 2006, p. 22). There are rising numbers of medical cases of neglect resulting in severe harm, injury, and death (FitzGerald, 2007).
Ø The government
Ø The California Correctional Peace Officers Associatio (CCPOA)
Ø The prison guards' union
Ø The Department of Corrections and Rehabilitation itself (CDCR)
The CDCR represents a sizable state agency that has been known to have its own agenda (Dumpel, 2006). For instance, press reports have recently shed light on some major underlying ethical issues with the CDCR such as the “code of silence” that is upheld by prison staff (Dumpel, 2006). In fact, each of the aforementioned bodies with their own area of responsibilities often have conflicting interests (Dumpel, 2006). The pursuit of their individual goals often results in the abuse of public trust and failure to meet the needs of inmates (Dumpel, 2006). In this highly political milieu, CDCR employees (including correctional RNs) strongly lack a meaningful voice within the system (Dumpel, 2006). To make matters worse, the poor condition of the system is exacerbated by the combination of these powerful interest groups and a heavily deficient budget (Dumpel, 2006). The pervasive lack of structure within government bodies that run health services create great challenges for those wishing to advocate for inmates and combat political forces that impact their rights to health care (Dumpel, 2006).
Several lawsuits against the CDCR outlined serious issues in areas such as (Dumpel, 2006):
Ø Improper screening of prisoners
Ø Staffing
Ø Incompetence with health care practices
Ø Access to care
Ø Medical records
Ø Implementing basic protocols
Ø Delays in care
Ø Pharmacy and medication management
Despite abundant legal action regarding prisoners’ health care in the past 20 years, it appears that “real and lasting improvements have yet to be achieved” (Dumpel, 2006, p. 22). There are rising numbers of medical cases of neglect resulting in severe harm, injury, and death (FitzGerald, 2007).
The History of Correctional RNs

http://prisonphotography.wordpress.com/
Following from this discussion on the history of correctional institutions, it is clear that the historical context of correctional nursing is strongly interwoven with that of the prisoners’ fight for proper health services. RNs have worked within prison walls since the late 1960s, and early 1970s (Dumpel, 2005). Since that time, the many inherent issues associated with correctional nursing have not been appropriately addressed, and thus are constantly rising within prisons (Dumpel, 2005). Needless to say, these challenges have seriously hampered correctional RNs’ role in providing safe, effective, therapeutic care to inmates, as well as to act as advocates towards their welfare (Dumpel, 2005).
The literature to date does not contain a significant body of knowledge regarding correctional nurses throughout the years, and thus the profession has yet to establish itself as a unique nursing specialty (Dumpel, 2005). Although administrators of health departments have addressed inmates’ needs and have set out health care standards for correctional facilities, they have, for the most part, ignored the central role that RNs play within these facilities, and generally refer to nursing in vague, general terms (Dumpel, 2005). This vagueness has been a major problem for RNs as they have been left vulnerable “to survive and function within the predominant influences of correctional facilities” (Dumpel, 2005, p. 27). These powerful forces within prisons create major role dilemmas for nurses as they must work in an environment where violence and attitudes of discrimination reign high amongst prison staff (Dumpel, 2005).
Despite U.S. laws stressing inmates’ rights to adequate health care, the lack of understanding and/or regard for such laws amongst prison staff and administration continues to be greatly problematic for RNs (Dumpel, 2005). There is a common attitude within prison culture that inmates are underserving of the same quality of health care that is offered to general society (Dumpel, 2005). As mentioned earlier, security is a chief priority within facilities, and thus administrators tend to prioritize measures of security, as opposed to defending and advocating for the role of RNs amongst staff (Dumpel, 2005). In fact, the correctional nurse is not usually considered “good” when advocating for and addressing the health needs of prisoners – they are seen as “good” when they assume a critical and disciplinary attitude towards inmates alongside the security staff while providing care (Dumpel, 2005).
The literature to date does not contain a significant body of knowledge regarding correctional nurses throughout the years, and thus the profession has yet to establish itself as a unique nursing specialty (Dumpel, 2005). Although administrators of health departments have addressed inmates’ needs and have set out health care standards for correctional facilities, they have, for the most part, ignored the central role that RNs play within these facilities, and generally refer to nursing in vague, general terms (Dumpel, 2005). This vagueness has been a major problem for RNs as they have been left vulnerable “to survive and function within the predominant influences of correctional facilities” (Dumpel, 2005, p. 27). These powerful forces within prisons create major role dilemmas for nurses as they must work in an environment where violence and attitudes of discrimination reign high amongst prison staff (Dumpel, 2005).
Despite U.S. laws stressing inmates’ rights to adequate health care, the lack of understanding and/or regard for such laws amongst prison staff and administration continues to be greatly problematic for RNs (Dumpel, 2005). There is a common attitude within prison culture that inmates are underserving of the same quality of health care that is offered to general society (Dumpel, 2005). As mentioned earlier, security is a chief priority within facilities, and thus administrators tend to prioritize measures of security, as opposed to defending and advocating for the role of RNs amongst staff (Dumpel, 2005). In fact, the correctional nurse is not usually considered “good” when advocating for and addressing the health needs of prisoners – they are seen as “good” when they assume a critical and disciplinary attitude towards inmates alongside the security staff while providing care (Dumpel, 2005).

http://prisonphotography.wordpress.com
| It is clear that the patient’s needs are always secondary to their punishment (FitzGerald, 2007). Improper medical management often prevent inmates from receiving their rightful medications, and nurses from legally adhering to the five rights of medication administration (FitzGerald, 2007). The consistent neglect of inmates’ health needs eventually brings them to the ER, for which taxpayers are paying hundreds of thousands of dollars (FitzGerald, 2007). This prevailing inefficient system is reflected in one correctional RN’s statement:
“You can’t have a caregiver and a jailer in the same body. It doesn’t work. The entire prison system favors punishment and incarceration. But as a nurse you are legally and morally bound to deliver care. But if the correctional system says, no, this guy is going into solitary, or this guy is going to be transported here or there, and he can’t take that pill or get that shot right now, corrections rules” (FitzGerald, 2007, p. 14). |
Correctional RNs as Executioners

http://www.executedtoday.com/2008/06/
In relation to the history of correctional nursing, it is noteworthy to mention that the recent movement of the American correctional system away from electric chairs and hooded executioners, towards lethal injections administered by health professionals, has had direct implications on correctional RNs (Holmes & Federman, 2003). In America, RNs and physicians are active participants in the death penalty procedures of inmates (Holmes & Federman, 2003). The U.S. provides both legal and identity protection to health care professionals involved in executions (Holmes & Federman, 2003).
This controversial nursing duty creates an obvious discrepancy between nurses’ roles as agents of care, and their state duty as administrators of the death penalty (Holmes & Federman, 2003). Thus, correctional nurses are confronted with many serious ethical dilemmas on a daily basis, lethal injections being arguably the most ethically questionable practice expected of them (Dumpel, 2006). It is known that within other nations, nurses may even have designated roles in the corporal punishment and torture of inmates (Holmes & Federman, 2003).
This controversial nursing duty creates an obvious discrepancy between nurses’ roles as agents of care, and their state duty as administrators of the death penalty (Holmes & Federman, 2003). Thus, correctional nurses are confronted with many serious ethical dilemmas on a daily basis, lethal injections being arguably the most ethically questionable practice expected of them (Dumpel, 2006). It is known that within other nations, nurses may even have designated roles in the corporal punishment and torture of inmates (Holmes & Federman, 2003).
The Future and Ongoing Shortage of Correctional RNs

http://articles.nydailynews.com/2010-09- 09/news/
As mentioned earlier, the population of prisoners in the correctional system more than tripled between 1980 and 1995 (Weiskopf, 2005). According to the Bureau of Justice Statistics Corrections Statistics, there were over two million prisoners in the U.S. in 2003 (Weiskopf, 2005). Furthermore, the inmate population is aging, due to “longer mandatory prison sentences and restrictive release policies, combined with the upward shift in the age distribution (Weiskopf, 2005, p. 337). These factors have together resulted in severely overcrowded conditions, and consequently in the growing demand and need for health care services within the correctional system (Weiskopf, 2005). Despite this upward trend in the inmate population, there has been little research in the area of health care delivery and nursing within prisons (Weiskopf, 2005).
In addition, it is known that prisoners’ health needs greatly exceed those of the general population (Dumpel, 2005). The competent skill set of correctional RNs are increasingly needed and are in critical shortage across correctional facilities due to numerous factors at play, many of which have been discussed throughout this historical overview of the profession (Dumpel, 2005):
Ø Aversion to working in a difficult, challenging, often hostile environment (Dumpel, 2005) Ø No proper recognition for the correctional nursing profession (Dumpel, 2005) Ø Advocating for prisoners continues to be burdened by personal risk to nurses themselves (Weiskopf, 2005) Ø Emotional burden of consistently confronting ethical issues of neglect of the prisoners (FitzGerald, 2007) Ø Outdated, old-fashioned system of management within correctional facilities (FitzGerald, 2007) Ø Lack of adequate resources to properly care for the inmates (FitzGerald, 2007) Ø Great lack of privacy, control and autonomy to carry out role as an advocate and health care provider (FitzGerald, 2007) Ø Constant discrimination and lack of respect from other prison staff (Dumpel, 2005) Ø Environment laden with violence and abuse, putting personal safety at risk (Dumpel, 2005) Ø While there was recent surge of interest, RNs quickly quit and leave the job as they soon experience these difficulties (FitzGerald, 2007) Altogether, as nurses have only been in correctional facilities since the late 1960s, their role in these environments is relatively new and evolving at a quick pace (Weiskopf, 2005). Despite the grim picture often painted for this area of nursing, the novelty of this profession leaves much room for improvement in the upcoming future. For instance, Norman and Parrish (1999) found that the traditional emphasis on the medical model of care within prisons is gradually now being replaced by a primary care model where interdisciplinary teams work together towards the welfare of inmates. As previously mentioned, there is still a great lack of national standards set up specifically for the field of correctional nursing (Dumpel, 2006). As such, it is imperative that leaders, experts, and educators are actively sought out in order to work collectively towards the establishment of solid curriculums within academic institutions, formal standards, and core functions that are specific to the correctional nursing environment (Dumpel, 2006). As once stated by Florence Nightingale; “Whatever else their imprisonment may do ‘it should do [the prisoners’] health no harm” (Willmott, 1997, p. 336). | 
http://hcpa.seiu.org/page/s/docnurses
|
